

Podcast: Newly approved drug may slow progression of Alzheimer’s
This episode of 'Show Me the Science' focuses on approval of a drug that attacks a key protein that contributes to dementia from Alzheimer’s disease
 Brian Gordon
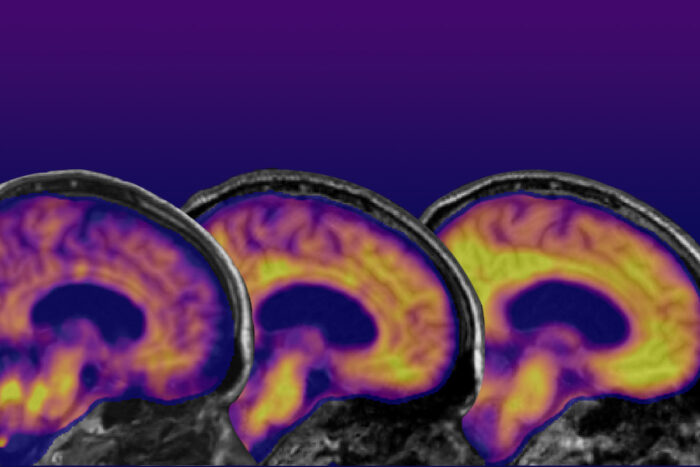
Brian GordonBrain scans of an Alzheimer’s patient taken over the course of years show growing areas of yellow, indicating the presence of the Alzheimer’s protein amyloid beta and reflecting its spread through the brain over time. In this podcast, Washington University researchers discuss the Food and Drug Administration’s recent full approval of the drug Leqembi (lecanemab) and what it could mean to the future of Alzheimer’s disease treatments. The drug is approved for use in people with mild dementia from the disease.
A new episode of our podcast, “Show Me the Science,” has been posted. These episodes feature stories about groundbreaking research, as well as lifesaving and just plain cool stuff involving faculty, staff and students at Washington University School of Medicine in St. Louis.
In this episode, Washington University researchers discuss the Food and Drug Administration’s recent full approval of the drug Leqembi (lecanemab) and what it could mean to the future of Alzheimer’s disease treatments. The drug is approved for use in people with mild dementia from Alzheimer’s disease, but researchers at Washington University’s Charles F. and Joanne Knight Alzheimer Disease Research Center (ADRC), believe the drug, along with other medications in clinical trials, one day may help prevent the development of memory loss and problems with thinking in people who have Alzheimer’s pathology in the brain but who have not yet developed clinical symptoms of the disease.
Barbara Joy Snider, MD, PhD, a professor of neurology and director of clinical trials at the Knight ADRC, says that although Leqembi doesn’t cure Alzheimer’s disease, it slows the decline in memory and thinking, and it also slows the progression of the disorder by removing some amyloid plaques from the brain.
John Morris, MD, director of the Knight ADRC, says with amyloid PET brain scans, blood tests and cerebrospinal fluid tests to detect problems before clinical symptoms of Alzheimer’s appear, it soon may be possible to delay or even prevent the development of Alzheimer’s dementia in some people at high risk.
The podcast, “Show Me the Science,” is produced by WashU Medicine Marketing & Communications at Washington University School of Medicine in St. Louis.
Transcript
Jim Dryden (host): Hello and welcome to “Show Me the Science,” conversations about science and health with the people of Washington University School of Medicine in St. Louis, Missouri, the Show-Me state. In this episode, the FDA recently has fully approved the first new treatment for Alzheimer’s disease that has been shown to slow the progression of the disease itself in people in the early stages of Alzheimer’s. Researchers at Washington University School of Medicine’s Charles F. and Joanne Knight Alzheimer Disease Research Center were among those who were involved in the clinical trials of the drug. Its brand name is Leqembi, and the drug also is known as lecanemab. It attacks the amyloid protein, one of the underlying causes of damage in the brains of patients with Alzheimer’s disease. The drug was approved to treat people who have mild disease, according to Dr. Joy Snider, a professor of neurology at Washington University and the director of clinical trials at the Knight Alzheimer Disease Research Center, also known as the ADRC.
B. Joy Snider, MD, PhD: This is the most exciting time we’ve had. The last meeting I went to in November, when these results were announced, there was palpable excitement throughout the crowd, and that never happened before at an Alzheimer meeting. So I think we’re all very excited about this drug and about this drug just being the beginning of new treatments for the disease.
Dryden: Snider is among the world leaders in Alzheimer’s disease research who recently gathered in Europe to discuss progress in the development of Alzheimer’s treatments as well as in the ability to detect Alzheimer’s disease earlier. She says Leqembi is unlikely to be the only drug approved that attacks the amyloid protein. Plus other treatments are being developed that work against another protein, called tau, which also is dysfunctional in patients with Alzheimer’s disease. And Dr. John Morris, the director of the Knight Alzheimer Disease Research Center, says better diagnostic tests also are being developed, many coming directly from work at the Knight ADRC.
John C. Morris, MD: I think these last few years have been just amazing in the progress in Alzheimer disease. When I began 40 years ago, 1983, working with the first director of the Knight Alzheimer Disease Research Center, Leonard Berg, I had no hope whatsoever that we would have a blood test to help diagnose a disease or a treatment that actually benefited patients by altering the Alzheimer disease process. So we need to keep going, but these are terrific developments.
Dryden: Damage in the brain can go on for two decades, maybe even longer, before a person finally develops clinical symptoms of Alzheimer’s disease. And Morris says much progress has been made in diagnosing the problem. For example, when he started in the field, it wasn’t possible to actually state with certainty that a person had Alzheimer’s disease until after they died and doctors looked at the brain under a microscope. Now researchers at the Knight ADRC have developed a test to detect amyloid in the blood. And they’re working on tests to detect the tau protein in cerebrospinal fluid. It’s also possible to detect Alzheimer’s-related brain changes with PET imaging in living patients even before symptoms arise. But until Leqembi recently was approved, it wasn’t clear that the ability to detect the disease earlier could really help patients, according to Dr. Joy Snider.
Snider: Leqembi has garnered a lot of attention for several reasons. The biggest one being it’s the first drug ever approved that changes the underlying biology of Alzheimer disease. We’re excited about it because it’s a drug that can alter the changes in the brain that happen with Alzheimer disease, and it does somewhat slow progression of the disease.
Dryden: That sort of answers my next question, which was: What makes this drug different from prior medications? But can you go a little bit more into that?
Morris: So prior drugs that are approved for the treatment of Alzheimer disease dementia only benefit the symptoms of dementia but do not alter the disease process. Those prior drugs don’t benefit people very much. This new drug alters the disease process and seems to slow the rate at which people with Alzheimer dementia progress. So it is a disease-modifying drug that has clinical benefit for patients.
Snider: To add to that, this drug affects the underlying brain disease in addition to slowing the progression of the symptoms. So that’s what’s different about it from any prior drugs that we’ve had.
Dryden: Who is eligible for this drug, and how is it given?
Snider: To be eligible for this drug, people need to have mild Alzheimer disease, which means they have memory symptoms, very, very mild memory symptoms, but they’re not severe. This drug was only tested in people with mild disease, and we don’t think, for a number of reasons, that it will help people with more severe disease. The reason to not just give it to everybody is because it has side effects. So like any drug, we only want to give it to people where it has benefits, so people with mild Alzheimer disease. This drug is given intravenously through an IV into your veins, and it’s given every two weeks. So it requires people to get an IV infusion every two weeks. Often, this would happen in an infusion center. In some cases, it might be done by a home health nurse, but that remains to be seen.
Dryden: Do you have an idea of what percentage of Alzheimer’s patients might be eligible for this drug or how long a person might be on the drug once it starts?
Morris: It probably would be about 15(%) to 20% of all people with Alzheimer dementia. So not the majority of individuals. It also is going to be difficult for many segments of the population to get access to the drug. It requires specialty, memory doctors. It requires an infusion center, requires sophisticated brain imaging to check for side effects, so this is not going to be easily accessible for many people. This is a big limitation because there will be eligible people who won’t have access to the drug.
Dryden: You mentioned side effects. What are they? Are they rare? Are they common?
Snider: There’s a couple of types of side effects. Some people have a reaction to the infusion. That’s pretty common, but usually very mild and usually something folks can deal with. They might feel a little anxious or short of breath, but usually those things are short-lived. The bigger side effects are the changes we see on brain imaging. So on the imaging that Dr. Morris was talking about, we can see changes in the brain that include small areas where the brain gets a little swollen like it had a bruise and also areas where there are small areas of bleeding called microhemorrhages. And those can happen with this drug in 20(%), 25% of people. In most cases, the people don’t even know it’s happened. They don’t have any symptoms. We just see it on imaging. And if we see that, we can make adjustments in the drug dosing. But some people, on the order of a few percent, can have more severe symptoms, can have headaches, confusion, stroke-like symptoms, things like that, and that can be pretty severe. That’s more likely to happen in people that have a certain gene called APOE4. So we will be testing for that gene when people think about taking the drug and then advising them on the risk, but those are the big risks.
Dryden: APOE4 is one of the first genes that was identified related to Alzheimer’s disease. So I would imagine that people who have APOE4 are probably the majority of people that you would see in the clinic?
Morris: Roughly half of people who have Alzheimer dementia will have at least one copy of this APOE4. Having that one copy doesn’t necessarily mean that one will develop Alzheimer dementia, but it certainly increases the risk of getting Alzheimer dementia. But we also have to recognize that about 50% of people who have Alzheimer dementia don’t have APOE4, so it’s not the only factor that causes the disease.
Snider: I would add to that that people with one copy of APOE4 may be at slightly higher risk of these side effects, but not a big effect. It’s the people with two copies that we have to really advise that the risk is higher. So those are the folks we’re going to be counseling and weighing the risk versus benefit of the drug even more carefully than usual.
Dryden: Leqembi is approved, but there also are other drugs that are in clinical trials for Alzheimer’s disease, even finishing clinical trials, correct? So what do you think is on the horizon when it comes to other drug treatments?
Morris: So we hope that the drugs that are currently being evaluated have even greater clinical benefit for patients, slow the rate of progression — ultimately, it’d be great if it would halt dementia progression. That would be terrific. Maybe have fewer side effects and maybe be much easier to administer rather than having an infusion every two weeks.
Snider: In the long term, we hope there will be choices, frequently or less frequent infusions, and also hopefully combination therapy. So maybe one drug isn’t enough to halt the progression of Alzheimer disease. Maybe we will need drugs that have multiple targets. So that’s what we’re looking forward to in the future is more studies looking at maybe adding on additional drugs and getting some drugs taken by mouth, which would be a lot easier.
Morris: As Dr. Snider indicated, for people who already have Alzheimer dementia, probably a single drug isn’t going to be as effective as a combination of drugs that address all of the brain pathology that causes Alzheimer’s disease. But what we really hope for is to use a drug or perhaps a combination of drugs in people who are at great risk of developing Alzheimer dementia but have not yet had memory changes or memory loss. That would be terrific because we could prevent dementia. So this drug and other drugs like it maybe, ultimately, have their greatest use in a treatment where it’s preventing Alzheimer dementia. That’s what we hope the future will bring.
Snider: And in fact, studies to see if that can happen are ongoing right now, both with this drug and with other drugs. So we are studying these drugs in people who don’t yet have symptoms but are at very high risk. Stay tuned; in another four or five years, we’ll get the results of those studies, and maybe we will have a preventive treatment.
Dryden: The Knight Alzheimer Disease Research Center here has been a world leader and the Dominantly Inherited Alzheimer Network, DIAN, has been examining, trying to understand the origins of Alzheimer’s disease and people with genetic mutations that almost guarantee that they’re going to have symptoms later on. The idea was to study those people to figure out what’s happening in the larger number of people who don’t have these inherited forms. I wonder, did that have anything to do with the development of this drug and other drugs down the pike? Or are those two completely separate questions?
Snider: So I think the DIAN observational study and the DIAN treatment study along with the studies done here at the Knight ADRC over the last 40 years really made the current drug studies possible, because they helped us develop the amyloid imaging PET scans, the blood tests, the spinal fluid tests, made all those things possible where we can tell who has Alzheimer disease for sure, if they have symptoms, and who’s at higher risk for it before they have symptoms. Right now, the DIAN treatment study has launched the first trial that actually does use two drugs. So they have a study where people are getting both an amyloid antibody — actually, same as Leqembi — as well as an antibody against tau. So that group is going to help us learn about how combination treatments can work as well.
Dryden: You mentioned amyloid and tau. Can you explain? Those are the two key proteins involved in the development of this disease, correct?
Snider: Those are the two key proteins that we see pathologically forming clumps in the brains of people with Alzheimer disease. They’re the proteins that Dr. Alzheimer saw over a hundred years ago under the microscope. We think they play a big role in the disease because they’re the pathology we can see, but we’re still really learning about exactly what does play a role in the disease.
Dryden: And she says, many investigational drugs are trying to address problems with amyloid, tau and other things that may contribute.
Snider: Many treatments target amyloid, some target tau, but there’s other treatments targeting the immune system, targeting other factors that might play a role. So there’s a lot of different ways to attack this disease. And that’s a good thing, because it’s a really complicated disease.
Morris: So amyloid and tau, as Dr. Snider indicated, are the hallmarks of Alzheimer’s, but there are many other changes that occur in the brain that may all need to be addressed by specific therapies. The current interest in anti-amyloid drugs is that current knowledge is the first abnormality that starts someone on the path to developing Alzheimer dementia is abnormality in how amyloid protein is metabolized. And so an anti-amyloid drug given very early may be the most effective way to prevent everything else that happens, including the onset of dementia. So again, we’re talking about prevention, but prevention at the very onset when we first notice that amyloid pathology is occurring. Treat them with an anti-amyloid therapy — hopefully that prevents the whole process including the development of dementia.
Dryden: And one of the things that has happened at the Knight ADRC is the development of tests, like blood tests, that might be able to detect those very first changes with amyloid.
Morris: Yes, it’s another amazing and very important development in our blood-based biomarkers to detect Alzheimer disease. I think, we all think, that as these biomarker tests become more widespread and better adopted, that will be an annual wellness visit for your Medicare. You’ll get your diabetes checked. You’ll get your kidney function checked, and you’ll get your blood test to see if you are on the path to Alzheimer disease.
Dryden: Will that be in time? I mean, I wonder if the wellness check needs to happen when somebody is 45 as opposed to 65.
Morris: We think that the changes that lead to the Alzheimer process probably begin in the 40s and 50s in most people. So it’s a long process because most people don’t develop dementia until they’re in their 70s. So we’re talking about a 20-year, 20-plus-year period where things build up before they cause dementia. So I think you’re right. I think the earlier we start screening, the better it would be if we have effective prevention strategies.
Dryden: Now back to this drug that’s been approved. Are there specific signs that might indicate that a particular patient might benefit from this particular drug?
Snider: What we know, based on the clinical trial, is that the drug can have benefit in people with very mild disease, and we measure that in a number of ways, but very, very mild memory symptoms. People that are otherwise healthy because most everybody who gets into a clinical trial is very healthy. And one of the important things that is happening with this drug is that we’re developing a patient registry that’s going to be national, and everybody on the drug will be entered in the registry. And we’ll be able to collect information on how well people do. And perhaps figure out who’s going to be the most likely to benefit down the line.
Morris: One problematic manifestation of drug trials is they almost all enroll people who are upper middle-class, white individuals. And so we don’t know how this drug or other drugs work in minoritized populations. We just don’t have that information. Do they get the same benefit or not? Do they have the same side effects or not? So we need to do a much better job of making these trials test their drugs in diverse populations. Treating Alzheimer’s disease in one group of people may not translate to treating Alzheimer’s disease in other groups, and people are now engaging in multiple strategies to try to improve diversity. We are holding a national conference here at the Knight ADRC in October to talk about enhancing participation from individuals from minoritized groups in Alzheimer research.
Dryden: What about cost? This is not going to be a cheap drug.
Morris: The Medicare coverage for the drug, the current idea is it may cover 80% of the treatment, but there’s a lot more that goes into it, including determining eligibility, which may require such things as a sophisticated imaging study called a PET scan. And then as Dr. Snider just mentioned, follow-up MRI scans once treatment is started to look for potential side effects. It’s not clear how all of that is going to be managed. I think the company that produced the drug said that something like a year’s treatment would be $26,000, something of that nature. If 80% of that is covered, that’s great, but we don’t know yet how long treatment should go. The trial showing the benefit went for 18 months. It’s not clear if we keep treating whether there will be more benefits. So a lot of things yet to discover.
Dryden: How long do you expect patients might have to take this drug, or do we know?
Snider: We don’t know. So the trial, I think Dr. Morris mentioned, was for 18 months’ treatment. But the people that were in that trial, many of them are still on the drug now a couple of years after the trial. That trial is ongoing for at least another two years. So we’re getting information about people’s long-term treatment on the drug, but we don’t know how long it’s needed.
Dryden: But however long it might be needed, it will be available at Barnes-Jewish Hospital in St. Louis, the hospital at which faculty at Washington University School of Medicine practice. The drug also has been approved to be used at hospitals throughout the BJC health system. Snider and Morris also expect other drugs to be approved as well, but as research moves forward, both say a lot more studies are needed.
“Show Me the Science” is a production of Wash U Medicine Marketing and Communications. The goal of this project is to introduce you to the groundbreaking research, lifesaving, and just plain cool stuff being done by faculty staff and students at the School of Medicine. If you’ve enjoyed what you’ve heard, please remember to subscribe and tell your friends. Thanks for tuning in. I’m Jim Dryden. Stay safe.


